OPINION -- Last week’s headline and article, “Oregon Ranks at the Bottom in Oral Health,” made three main points.
First, public and private funders are collaborating to help Oregon kids get more access to professional dental care. This is very good news. No one wants kids, or adults, to suffer from bad teeth, and everyone involved in this work deserves a lot of credit.
Unfortunately, the other two main points - Oregonians have the worst teeth in the country and water fluoridation is the most effective (and cost-effective) way to address the problem – are simply wrong.
Let’s set the record straight, starting with the oft-repeated claim that “For every $1 spent on water fluoridation, an average of $38 is saved on dental treatment costs per person per year.” This comes from one 2001 paper by Griffin et al and has been touted as gospel by fluoridation promoters ever since.
But last year, Griffin’s paper was thoroughly rebutted by the Lo/Thiessen study, which calculated no such savings. It determined that Griffin underestimated actual fluoridation equipment, repair and employee expenses ($7-$9 per hour labor costs?) and omitted any costs for related health problems caused by fluoridation chemicals, such as treatment for fluorosis.
For oral health, let’s use two measurements that have data for most or all states. For kids, survey dates can vary. For adults, all figures are 2012. According to the CDC’s Oral Health Division, Oregon ranked 29th in third grade children in having at least one cavity – not great, but hardly at the bottom. Oregon’s rate was 57.5%, close to the national average of 54.2%.
For adults 65 and older who have lost six or more teeth due to tooth decay or gum disease, Oregon’s rate, 34.7%, ranked 10th best in the country.
Only 23% of the state is fluoridated, ranking us 48th in the country. Government and the American Dental Association consistently try to blame high cavity rates on lack of fluoridation. To recap, virtually no such causation, or even correlation, exists:
Fluoridation: 48th
Childhood oral health: 29th
Adult oral health: 10th
Indeed, solid evidence of fluoridation’s ineffectiveness is deep and wide:
- In 1990, the largest U.S. study by the National Institute of Dental Research found that children drinking fluoridated water averaged only about half a cavity less than those drinking unfluoridated water.
- In 1999, CDC acknowledged that fluoride’s “actions are primarily topical for both adults and children,” meaning surface applications like toothpaste
- Today, CDC, a major fluoridation promoter, says that fluoridation reduces cavities in children by 25%. Again, this is less than one cavity per child for an entire childhood.
- The Iowa Study, funded by the National Institutes of Health, is the most comprehensive ongoing fluoride research project in the U.S. It found “The benefits of fluoride are mostly topical . . . findings suggest that achieving a caries-free status may have relatively little to do with fluoride intake (emphasis in the original) . . . recommending an ‘optimal’ fluoride intake is problematic.”
Then there’s the Cochrane Collaboration, an independent organization of more than 37,000 medical and scientific volunteers in more than 130 countries. Its research is based on the principles of evidence-based medicine and it’s considered the gold standard of evaluating effectiveness.
Cochrane cited solid scientific data finding topical applications like sealants and varnish to be effective in two 2013 studies, but in 2015, it found virtually no such credible evidence for fluoridation:
“The available data come predominantly from studies conducted prior to 1975 . . . over 97% of the 155 studies were at a high risk of bias, which reduces the overall quality of the results . . . We did not identify any evidence . . . to determine the effectiveness of water fluoridation for preventing caries in adults . . . There is insufficient evidence to determine whether water fluoridation results in a change in disparities in caries levels across socio-economic status.”
Promoters invariably argue fluoridation helps low-income kids, but Cochrane found no credible studies indicating this. In fact, there has never been a randomized, controlled study of fluoridation to determine safety and effectiveness.
On-the- ground experiences in cities like Boston, New York, Cincinnati and Pittsburgh provide more evidence. For instance, San Antonio reported in 2011 that “After 9 years and $3 million of adding fluoride, research shows tooth decay hasn’t dropped among the poorest of Bexar County’s children. It has only increased – up 13 percent this year.”
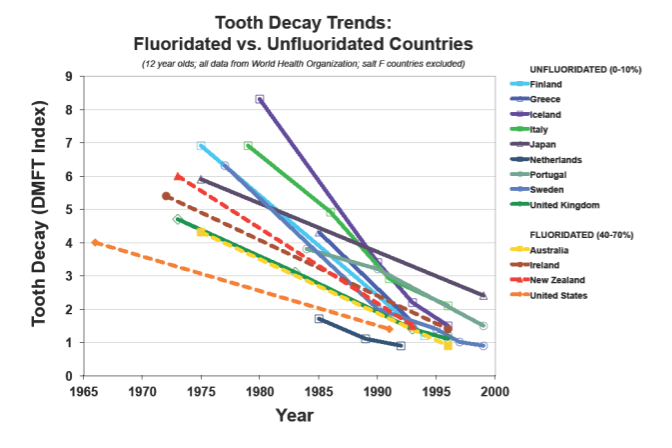
Finally, the ineffectiveness is apparent worldwide. A World Health Organization study found that nations that fluoridate have virtually the same cavity rates in children as nations that don’t (see graph compiled from WHO data below).
Several factors have major effects on dental health, especially diet, personal dental habits, professional care and genetics. But based on a wealth of credible data, fluoridation isn’t one of them.
This is only part of the story. The other major components are fluoridation’s health risks and dubious ethics. To be continued . . .
Rick North is the former executive vice president of the Oregon American Cancer Society (1993-1998) and former project director of the Oregon Physicians for Social Responsibility’s Campaign for Safe Food. He retired from PSR in 2011 to become a volunteer addressing threats to the environment, food and water safety, and our democracy.
Comments
It's the facts that matter
It's the facts that matter and Mr. North pointed out convincingly "with facts" that Oregon is not at the bottom of states in terms of oral health which was clearly wrong in the previous Lund article. It's those facts and evidence that Mr. North cited that readers will trust.
Michael Framson
Fluoridation is a Failed Concept
First, the Lousiana report (not peer-reviewed published study) "Billy Budd" uses as proof that fluoridation reduces tooth decay has many limitations that the CDC described 16 years ago, when it was first published using now-20-year-old statistics. Today an astonishing number - 62% - of Louisiana's third graders have tooth decay.
Second, the New York State Study, "Billy Budd" cites was written by a pro-fluoridation activist who used Medicaid dental costs as a basis of his report. However, most dentists in New York State won't treat Medicaid patients who then must get care when they are in severe dental stress which would not be classified as dental decay - but infection, abscess or other non-dental classification. This paper has many other flaws, also
Third, Billy Budd's cut and paste was probably posted without even reading Rick North's article since Bill Budd included Oregon as proving fluoridation is effective which Rich North has already debunked in his article
Tooth decay crises are occurring in all fluoridated cities, states and countries. See http://www.FluorideNews.Blogspot.com
Severe tooth decay is responsible for 2/3 of hospital visits by children under six in New York State (1), where almost 73% of the population drinks fluoridated water. Even in 100% fluoridated New York City, more children required cavity-related hospitalizations, proportionately, than two of New York State's largest non-fluoridated counties, Suffolk and Nassau, whether payment was made by Medicaid or privately.
One New York City hospital charged from $929 to $12,199 to treat 96 children with severely decayed teeth, excluding the dentist and anesthesiologist fees. Children needed extensive work including stainless steel crowns, extractions, root canal therapy, fillings, other restorations, periodontal procedures, surgeries and/or more.
New York State hospital charges for the 2,726 early childhood cavities-related surgical visits required by children under six, in 1999, lie anywhere between $2.5 and $33 million, report NYS Department of Health Dentists, Kumar and Green, and others, in the Winter 2003 Journal of Public Health Dentistry, who also report they may be underestimating the numbers of children so treated.
Even after hospital treatment, these children return with new lesions, say Kumar and colleagues.
This is how Jonathan Kozol explains it in his book Savage Inequalities about life in the fluoridated South Bronx, in New York City: “Bleeding gums, impacted teeth and rotting teeth are routine matters for children..... Children live for months with pain that grown-ups would find unendurable. …I have seen children with teeth that look like brownish, broken sticks. I have seen teenagers who were missing half their teeth....”
References: http://fluoridedangers.blogspot.com/2005_11_01_archive.html
Nys Cof
World Health Organization data
Dr. Ferre is correct that the World Health Organization didn’t do a formal study on cavity rates in various countries. My wording wasn't entirely accurate on that. However, WHO did gather and publish the data. The graph from that data clearly shows virtually no difference in cavity rates between fluoridated and unfluoridated nations. The author of your citation supposedly in opposition didn't question that or the accuracy of the graph, but only different interpretations of it. I'll repeat what I said in response to Dr. Slott, who's using the same information you have: Add up the evidence of fluoridation’s minimal effectiveness: Oregon’s rankings, the Ko/Thiessen study, the NIDR and CDC’s figures, the Iowa Study (where the lead author himself found effectiveness even less than the CDC), the Cochrane Report, the experience of numerous U.S. cities and the international WHO data shown in the graph. No one study or report may be definitive, but taken together, it’s a compelling picture. I stand firmly by my conclusions that Oregon is NOT at the bottom in oral health (by one measure of adult oral health, it's near the top), it doesn't save money, and it's minimally effective. I’m glad that Oregon is pursuing far more effective alternative oral health measures such as getting more low-income kids professional dental care. That’s something we can all support.
Rick North
What the World Health Organization says about fluoridation:
Mr. North: Finally, the ineffectiveness is apparent worldwide. A World Health Organization study found that nations that fluoridate have virtually the same cavity rates in children as nations that don’t (see graph compiled from WHO data below).
Facts:
There is no "World Health Organization study" which finds any such thing. To what North refers is a skewed interpretation of WHO data by Fluoride Action Network (FAN), not what was reported in any WHO study. The graph he presents is not one prepared by WHO. It is a graph prepared by Chris Neurath of FAN which depicts the skewed misrepresentation of WHO data.
Ken Perrott, a Biochemical PhD in New Zealand has written an excellent description of this misinformation on his website "Open Parachute".
The first formal WHO Guideline for fluoride in drinking water was established in 1984 in the first edition of its Guidelines for drinking water quality. (The World Health Organization defines the Guideline Value as "the concentration that does not result inany signiicant risk to health over a lifetime of consumption"). A guideline value of 1.5 mg/litre was set for fluoride. All subsequent editions have retained 1.5 mg/litre as the guideline value for fluoride.
Guidelines for drinking water quality recommends that:
“In setting national standards for fluoride or in evaluating the possible health consequences of exposure to fluoride, it is essential to consider intake of water by the population of interest and the intake of fluoride from other sources (e.g., from food, air and dental preparations). Where the intakes from other sources are likely to approach, or be greater than, 6 mg/day, it would be appropriate to consider setting standards at a lower concentration than the guideline value.”
However, for optimal dental health WHO suggests a lower level of fluoride of between 0.5 and 1.0 mg/liter, and recommends that where caries rates are moderate to high, or where there is evidence of increasing caries rates, fluoride levels should be increased to this optimal level (World Health Organization Expert Committee on Oral Health Status and Fluoride Use 1994).
The optimal level today is 0.7 mg/l or parts per million (ppm). Over 211 million Americans today enjoy the public health benefit of fluoridation.
Dr. Kurt Ferre
missing the point
Reader Billy Budd seems to be missing the point. The first point he misses is that the data claiming effectiveness of adding fluoridation chemicals to public water supplies is tainted, just like the water itself. But the even bigger point is this: while the benefits of fluoride are in question at best, there can be no doubt as to its potential and demonstrated harmful effects. As with all other drugs, fluoride affects different people in different ways. A specific dosage may have absolutely no effect on one person (positive or negative), yet this dosage may very beneficial to another, and yet still be lethal to someone else. (And we won't even mention the issue of an uncontrolled dosage!) Take Thalidomide for example. While it was very effective and useful for hundreds of thousands or maybe millions of people, it had drastic and dire consequences for tens of thousands of others. So the question is this. Is it ethically permissible to administer a known toxin to a large number of people because it (allegedly) has potential benefits for a few? Unlike Thalidomide, whose victims took the drug by their own choice even though they had been misled by false claims, administering a drug through the water supply leaves people with no practical choice. You either move out of town, or install a very costly filtering system. On the other hand, by making fluoride an "opt-in" choice, those who believe in its health benefit claims can easily make a guinea pig of themselves if they so desire.
Brian Perkins
No point missed
Nothing could be further from the truth with respect to this claim of "tainted water." These misguided and mistaken pieces of fear-based propaganda are what is causing cavities when average people mistakenly reject fluoridation.
In fact fluoridation water additives must meet very strict and well defined purity tests which are even more specific, more transparent and more verified than the USP standard which applies to drugs.
see:
http://www.cdc.gov/fluoridation/factsheets/engineering/wfadditives.htm#a9
Information on a comparison between the National Sanitation Foundation standards and USP is about 2/3rds down the page.
Quality control testing shows that save for arsenic, contaminants are not detectable in the vast majority of samples.
http://www.nsf.org/newsroom_pdf/NSF_Fact_Sheet_on_Fluoridation.pdf
The tiny bit of arsenic detected is about 2/1000 of that present in the average American's daily diet and far far below what the EPA has determined to be safe for human health.
see:
Arsenic from community water fluoridation: quantifying the effect. E Peterson, et al. Journal of Water and Health (In Press) 2015
Dietary Reference Intakes, The National Academies Press 2001
This is too small an amount to possibly have any harmful effect.
Why a community would choose to put its faith in the opinions of people like Mr. North rather than America's pediatricians, family physicians, internal medicine specialists, and public health scientists is beyond understanding.
Fluoridation simply prevents cavities.
Billy Budd
Obfuscation
NYSCOF's "reply" to my post is classic obfuscation. Sadly, a great deal of knowledge is necessary to catch what is wrong.
1. The Louisiana study was from the CDC's oral health divisions and published in the internationally recognized Morbidity and Mortality Weekly Report. All materials there are submitted to an extensive peer review process of the most sophisticated sort. Other divisions in the CDC review all these publications. The review is sufficient to warrant inclusion in the National Library of Medicine's database. The magazine Fluoride where much of the materials which oppose community water fluoridation is found lacks such peer review and is not listed by PubMed in the NLM database. These data have also been in other journal articles.
For example: J Public Health Dent. 2000 Winter;60(1):21-7. Dental services, costs, and factors associated with hospitalization for Medicaid eligible. children, Louisiana 1996-97. Griffin SO, et al
2. This discussion is about severe early childhood caries, not about average caries incidence, a statistic that is insensitive to fluoridation's benefits. The Oregon data has not been published but was gathered by an Oregon Pediatric Dentist and can be viewed in graphic form here:
http://photos.oregonlive.com/photogallery/2015/05/fluoridation_prevents_children.html
3. The even more current literature confirms 1999 study of a 50% decrease in Medicaid bills from fluoridation.
see JADA article below for example and:
Br Dent J. 2014 Mar;216(5):E10. doi: 10.1038/sj.bdj.2014.180. An alternative marker for the effectiveness of water fluoridation: hospital extraction rates for dental decay, a two-region study. Elmer TB et al
3. That there are cavities despite fluoridation is a classic straw man argument. The science clearly demonstrates there would be even more without the protection fluoridation creates. Edelstein, the senior author of the recent New York study is one of the most prestigious oral health scientists in the world. He found that fluoridation saves New York City about $56,000,000 over 10 years in Medicaid Bills for children 6 and under.
Reducing early childhood caries in a Medicaid population. Edelstein et al Journal of the American Dental Association Volume 146, Issue 4, Pages 224-232, 2015 http://jada.ada.org/article/S0002-8177(15)00221-4/abstract
4. Wary readers should remember the easily verifiable fact of the overwhelming scientific consensus among real experts is that fluoridation prevents cavities, is important, save and inexpensive. About 150 professional, scientific and health advocacy organizations recognizing fluoridation's importance to oral public health are listed by the Quebec National Institute of Public Health.
http://www.inspq.qc.ca/pdf/publications/705-WaterFluoration.pdf p 47
Rather than believing misleadingly constructed graphs readers should actually read the group Platform for Better Oral Health in Europe has written confirming fluoridation's effectiveness.
http://www.oralhealthplatform.eu/wp-content/uploads/2015/10/Best-practices-collection.pdf
Clearly while NYSCOF, FAN, "Dr" Mercola, and Natural News, four of the most prominent fluoridation opponents, often are successful in convincing lay citizens, the expert scientific community sees past the cherry picking, straw man arguments and mistaken conclusions.
The Oregon Health Authority is one such group of experts whose State Health Improvement Plan calls for increasing fluoridation to 80% in Oregon.
Billy Budd
Dental insurance reform?
For perspective on the effect healthcare reform may have on dental insurance, find more at: http://www.healthcaretownhall.com/?p=6038
Jeremy Engdahl-Johnson
There is a mature and unopposed literature showing the fluoridation more than pays for itself even if only the effect on baby teeth are considered.
About 2/3rds of the operations on little preschool kids are avoided. These procedures under general anesthsia include extractions, root canals and unsightly stainless steel crowns. Fluoridation's remarkable effect in decreasing these operations has been documented in Australia, England, Scotland, Texas, New York, Louisianna and Oregon.
See for example: Water Fluoridation and Costs of Medicaid Treatment for Dental Decay -- Louisiana, 1995-1996. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention September 03, 1999 / 48(34);753-757 http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4834a2.htm
Readers need to decide if they are to believe Mr. North, who once worked for the Oregon Cancer Society or North America's pediatricians, family physicians and internal medicine specialists.
America's pediatricians through their society, the American Academy of Pediatrics, state the truth:
"Fluoride plays a very important role in the prevention of dental caries. Although the primary mechanism of action of fluoride in preventing dental caries is topical, systemic mechanisms are also important. "
"Water fluoridation is a cost-effective means of preventing dental caries, with the lifetime cost per person equaling less than the cost of 1 dental restoration. In short, fluoridated water is the cheapest and most effective way to deliver anticaries benefits to
communities."
Billy Budd