The Oregon Health Authority is changing its approach to Medicaid to improve health and contain costs.
July 19, 2018
Image
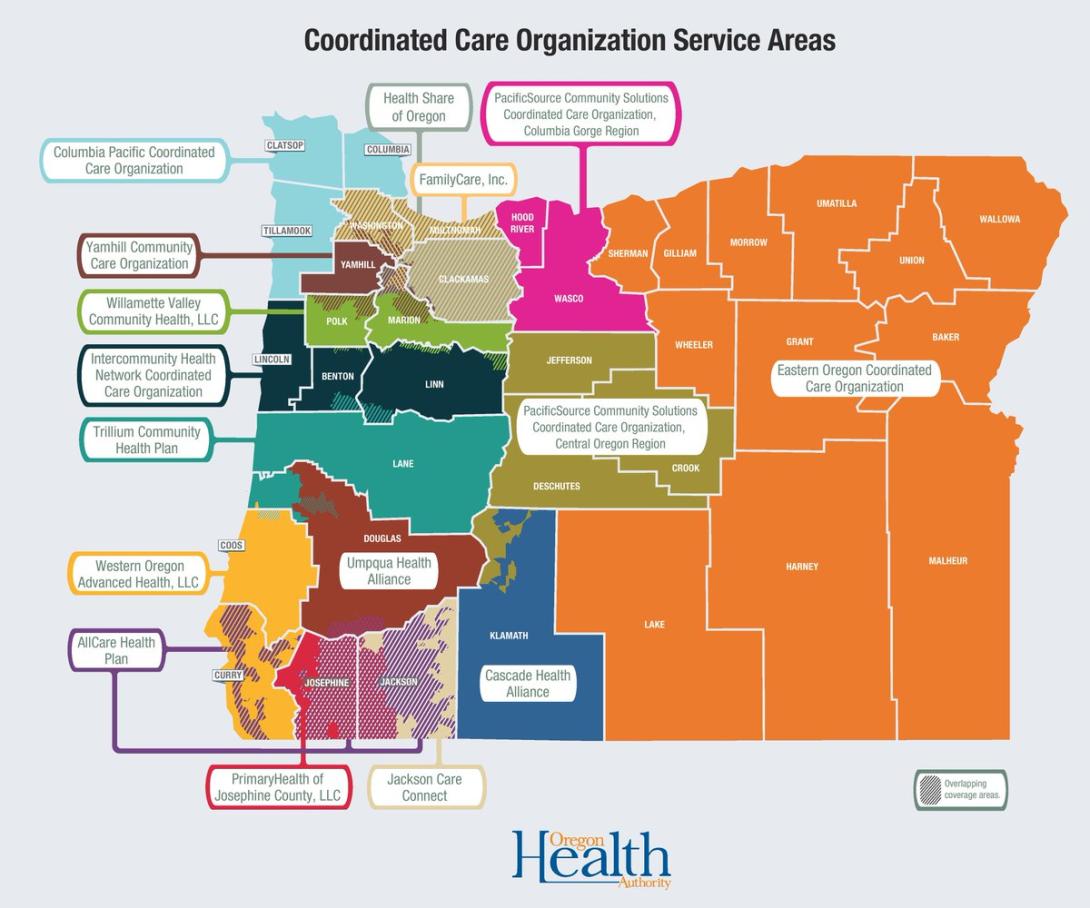
Current service areas for Oregon's coordinated care organizations.
|
OREGON HEALTH AUTHORITY
Oregon’s facing an $8 billion question: Can state bureaucrats and politicians reinvent the health insurance program that covers one in four Oregoni
